Manufacturer > Cardiovascular Systems > Devices > DIAMONDBACK 360® PERIPHERAL ORBITAL ATHERECTOMY SYSTEM
DIAMONDBACK 360® PERIPHERAL ORBITAL ATHERECTOMY SYSTEM

Expand your PAD treatment options with multiple access solutions and low profile advantages of the revolutionary Diamondback 360 Peripheral Orbital Atherectomy device. The low profile design facilitates minimally invasive treatment options for those with peripheral artery disease.
In multiple clinical studies with real-world patients and the most challenging lesions, OAS has demonstrated successful lesion modification while maintaining low complication rates.
Features and Benefits
OAS is a Solution for Arterial Calcium
When treating peripheral artery disease (PAD), even with angiography, peripheral calcium tends to be underestimated.9 And studies show that calcium negatively affects patient outcomes.
PATIENT PREDICTORS OF ARTERIAL CALCIFICATION
- Diabetes
- Chronic Kidney Disease
- Advanced Age (>65 y/o)
- Smoker
- Dyslipidemia
- Hypertension
- Prior CABG
- Known PAD/CAD
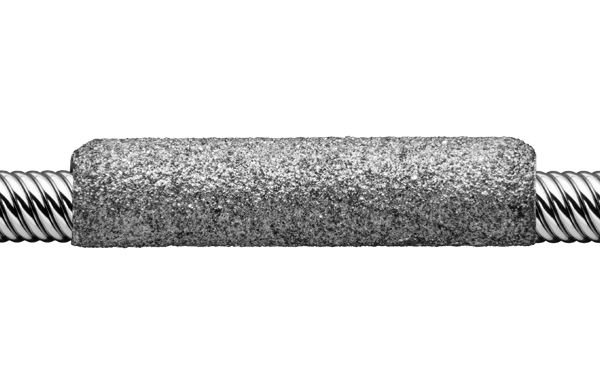
Solid Crown
- The mass of the crown is designed for maximum calcium removal
- Diamond-coated surface area allows for short run times
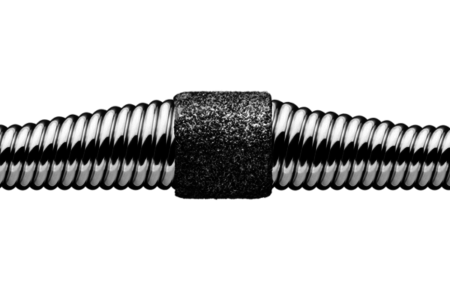
Classic Crown
- The most flexible of our crown configurations.
- Designed for vessel bends, ostial lesions and distal below-the-knee procedures
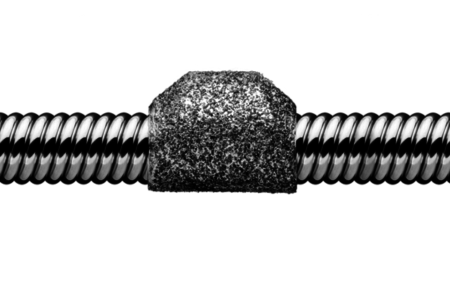
Micro Crown
- Designed with flexibility for tortuous vessels and tight bends below-the-knee
- GlideAssist mode for the 1.25 Micro Crown enables the crown to spin at a slow speed (5k RPM) for easier tracking and removal of the device over the guide wire.
Use Case Examples
THREE VESSEL TREATMENT FOR PAD
Overview
Dr. Sadeem Mahmood used orbital atherectomy in the treatment of multi-stage vessel disease.
Patient History
An 88-year-old female complained of bilateral lower extremity pain with exercise and right lower extremity pain at rest. After multiple antegrade access attempts, retrograde access was achieved under ultrasound guidance and successful Orbital Atherectomy System (OAS) treatment of multi-stage vessel disease was performed.
Patient presented with bilateral lower extremity pain with exercise and right lower extremity pain at rest. She was diagnosed with Peripheral Arterial Disease (PAD) and classified as Rutherford category 4 with past medical history of diabetes mellitus, renal insufficiency, hypertension and coronary artery disease. An angiogram revealed 80% stenosis in the right superficial femoral artery, 75% stenosis in the proximal popliteal artery and 100% stenosis [chronic total occlusion (CTO)] of the right anterior tibial artery.*
Treatment Summary
4 Fr. 60cm Diamondback 360® Peripheral Orbital Atherectomy System (OAS) facilitated retrograde treatment of multi-vessel disease.
Retrograde access of the right anterior artery was successfully achieved using ultrasound guidance after multiple failed attempts to cross the lesion through the antegrade approach. A 60cm Diamondback 360® Peripheral 1.25mm Solid Crown was used for retrograde orbital atherectomy treatment of lesions in the right anterior tibial, popliteal, and superficial femoral arteries. Lesions were treated with low, medium, and high speed OAS passes. This was followed by low-pressure percutaneous transluminal angioplasty (PTA) at 6 ATM in each of the lesions treated. PTA was also used to treat the tibial peroneal trunk and peroneal artery through an antegrade approach.
Key Takeaways
Final results showed less than 5% residual stenosis in all target lesions. Excellent blood flow to the foot was present. No complications occurred and the patient was discharged on the same day.
- Diamondback 360® 60cm device facilitated treatment of multiple vessels through 4 Fr. platform.
- Retrograde access through the right anterior tibial artery was successfully achieved after multiple attempts to cross the lesion from an antegrade approach.
- OAS and low-pressure adjunctive balloon angioplasty procedures resulted in less than 5% residual stenosis in all target lesions with no complications.
RETROGRADE TREATMENT IN THREE VESSELS
Overview
Dr. Howard J. Feldman used orbital atherectomy to improve distal flow in a Peripheral Artery Disease (PAD) patient with diffuse and densely calcified disease.
Patient History
A 73-year-old male with critical limb ischemia (the most severe form of PAD) and chronic total occlusion (CTO) presented with non-healing ulcers on his right toes and associated osteomyelitis of the right second toe. After a failed antegrade approach, successful retrograde access was achieved through the right anterior tibial artery allowing for treatment of diffuse and densely calcified disease in three vessels.
This Rutherford category 5 patient had multiple risk factors for peripheral artery disease. He was a poorly controlled Type 2 diabetic who continued to use tobacco. Medical history also included hypertension, hyperlipidemia, ischemic heart disease with prior coronary artery bypass grafting (CABG), peripheral neuropathy, and chronic obstructive pulmonary disease (COPD). Previously, he underwent a right common femoral endarterectomy with bilateral femoral popliteal bypasses. A second left femoral popliteal bypass was performed two months after the initial procedure.
Pre-atherectomy assessment showed the right dorsalis pedis pulse to be detectable by Doppler while the right posterior tibial pulse was absent. Angiography revealed CTO of the right femoral popliteal bypass graft, a patent right profunda femoris artery, and a diffuse and densely calcified CTO of the right superficial femoral artery (SFA) extending below the knee into the popliteal artery.*
Treatment Summary
Through retrograde access, a 4 Fr. 60 cm Diamondback 360® Peripheral Orbital Atherectomy System improved distal flow in a Peripheral Artery Disease (PAD) patient with diffuse and densely calcified disease.
Initially, antegrade crossing of the right SFA CTO was attempted but was unsuccessful. Retrograde crossing was then attempted under ultrasound guidance. Retrograde angiography via an anterior tibial access revealed a diffusely diseased anterior tibial (AT) artery and densely calcified subtotal occlusion to CTO of the tibial-peroneal trunk (TPT) and peroneal arteries.
Retrograde anterior tibial access was achieved and a .012″ ViperWire guide wire was advanced across the lesion to the distal right popliteal artery. Orbital atherectomy treatment was completed in three different vessels with a 4 Fr. 60 cm Diamondback 360® 1.25 mm Micro Crown. Since the patient had diffuse disease, multiple lesions were treated within each vessel. The anterior tibial artery was treated followed by the tibial-peroneal trunk and peroneal arteries. Low pressure percutaneous transluminal angioplasty (PTA) was then performed at 6 ATM and 4 ATM in the right peroneal and right anterior tibial arteries, respectively.
Key Takeaways
Orbital atherectomy facilitated reduction in the ostial right anterior tibial artery stenosis from >80% to 0% and reduction in the proximal right peroneal artery stenosis from 95% to <30%. Post-procedural flow was sufficiently enhanced to render retrograde luminal opacification suboptimal. Additionally, the dorsalis pedis Doppler signal changed from monophasic and severely damped prior to treatment to strong and biphasic post-intervention. With improved distal flow to the right foot, the patient was referred for a femoral tibial bypass graft surgery.
- Successful retrograde access through the right anterior tibial artery was achieved after failing to cross the CTO from an antegrade approach.
- The unique mechanism of action of orbital atherectomy and the low profile 4 Fr. 60 cm Diamondback 360® 1.25 mm Micro Crown facilitated treatment of three vessel disease.
RETROGRADE TREATMENT USING 60CM DEVICE
Overview
Dr. Mehiar El-Hamdani used orbital atherectomy in the treatment of a severely calcified below the knee TPT stenosis.
Patient History
This 67-year-old caucasian male is a self-employed bar owner who spends long hours on his feet. He presented with severe leg pain while walking and severe rest pain.
The patient had a history of peripheral artery disease (PAD), neuropathy, diabetes, coronary artery disease, hypertension, and hyperlipidemia. He has smoked 3 to 4 packs per day for the past 47 years. Rutherford classification was category 4 due to rest pain.
Prior treatments for PAD (including a non-healing right leg ulcer of 2 to 3 months duration) included above the knee balloon angioplasty and stent placement in the left superficial femoral artery (SFA) in August 2013 and the left and right common iliac arteries in July 2013. The right leg ulcer healed completely but the patient continued to complain of claudication mainly in the left leg. Walking was limited to less than 100 yards.
Assessment prior to atherectomy showed a severely calcified lesion in the TPT, which was 80 mm long and 80% stenosed. Severe disease was also noted in the popliteal artery and the superficial femoral artery (SFA) with in-stent restenosis (ISR).
Treatment Summary
Retrograde anterior tibial artery access with a 60 cm Diamondback 360® 1.25 mm Solid Crown resulted in reduction of a tibial peroneal trunk (TPT) stenosis from 85% to 0%. The orbital atherectomy procedure was completed quickly in 11 minutes.
Prior to treating below-the-knee lesions with orbital atherectomy, the patient underwent endovascular treatment for inflow disease. After accessing the anterior tibial artery via ultrasound guidance and treating inflow disease through a 6 Fr sheath, a guidewire was used to cross the TPT lesion and advanced down into the posterior tibial artery from the sheath placed in the distal anterior tibial artery. After exchange of the Asahi Regalia for a 0.012″ CSI ViperWire®, orbital atherectomy was carried out using a 60 cm Diamondback 360® Peripheral Device 1.25 mm Solid Crown. The initial pass of the crown was at low speed for 30 seconds. This was followed by two additional passes, one at medium speed for 15 seconds and a final pass at high speed for 20 seconds.
After orbital atherectomy of the TPT, balloon dilatation was performed using a 4.0 mm x 80 mm Chocolate® Balloon [TriReme Medical] at 6 ATM for 3 minutes. No waist was observed in the balloon.
Total procedure time for the retrograde anterior tibial artery approach and treatment of the TPT was approximately 11 minutes, which included passing and exchange of the guide wires, access of the TPT lesion, atherectomy, and post-atherectomy balloon angioplasty.
Key Takeaways
After Diamondback Peripheral Orbital Atherectomy and adjunctive PTA, residual stenosis in the TPT was 0%. The patient was discharged to home 8 hours after the procedure. Rest pain resolved, and the patient was able to walk further without experiencing claudication.
ULTRASOUND GUIDED TREATMENT
Overview
Dr. Jihad Mustapha used orbital atherectomy in the unique treatment of three vessel disease.
Patient History
A 72-year old female patient, fully independent, retired with a goal to be more active with her husband, was complaining of pain at rest in her left leg. Patient was treated using ultrasound-guided tibiopedal access and the total procedure time was 20 minutes.
Over the previous few months, the patient’s claudication symptoms had caused her to limit physical activity and she was experiencing left leg pain at rest. Past medical history included diabetes mellitus, hypertension, hyperlipidemia, and chronic renal disease (stage III).
She did not have a previous history of peripheral or coronary artery disease. She was classified as Rutherford category 4. An angiogram revealed stenosis in the left superficial femoral, popliteal, and anterior tibial arteries.
Treatment Summary
4 Fr. Diamondback 360® Orbital Atherectomy System allowed for unique retrograde treatment approach of three vessel disease.
Using ultrasound guidance, retrograde access was gained through the left anterior tibial artery with a 4 Fr. sheath. An 0.012″* ViperWire® was advanced through the left anterior tibial artery followed by crossing of the popliteal and superficial femoral arteries. A single, 60 cm* Diamondback 360® 1.25 mm Micro Crown was used for retrograde treatment of all three lesions in the superficial femoral, popliteal and anterior tibial arteries. Each lesion was treated using two passes on low and two passes on medium speed with OAS. Low pressure adjunctive balloon angioplasty was performed at 4 ATM for 2 minutes in each lesion. Total procedure time was less than 20 minutes, radiation time was 4 minutes and only 16 cc of contrast was used.
Key Takeaways
- Total procedure time was less than 20 minutes
- Patient was discharged the same day and walked out of the hospital in less than 2 hours post-procedure
- Total radiation time was 4 minutes
- Total contrast used was 16 cc
- OAS has a unique mechanism of action that can allow you to treat multiple vessels with one crown, and also has the option for smaller sheaths
